Darwinian Evolution of Cancer
Recognizing the Darwinian Evolution of Cancer is essential for understanding the main problem we have in treating malignant (cancerous) metastatic tumors, the resistance and recurrence of the disease, and in most cases death from it. However, the knowledge of the Darwinian Evolution of cancer is also humanity's strongest weapon to one day achieve the cure for metastatic cancer.
Gatenby emphasizes “all populations evolve to adapt as well as possible to the existing environment, but except for humans, none of the other living beings can ever predict the future. Scientists and oncologists can predict the future because we know evolution. Knowing evolution is what will enable us to develop therapies that will one day achieve success in the clinic”.
Natural Selection is the process through which Nature selects inheritable physical and functional traits in offspring that ensure the best fit for the current environment. Applying the ideas developed by Darwin to explain the origin of species helps us understand the beginning and development of cancer (carcinogenesis) and the best strategies for its treatment.
As a result of the action of Natural Evolution and Natural Selection specific to a given environment, there will be the development, the best possible perfection for the current conditions of the microenvironment in structure and function, for normal cells; whereas for pathological cells, it is the development of cells with the most aggressive traits, the development of resistance to the unfavorable conditions of the microenvironment and against treatment (the goal is survival/space occupation/reproduction).
When talking about tumors, the entire discussion is about malignant metastatic tumors, metastatic cancer. With rare exceptions, it is incurable. All truly non-metastatic malignant tumors, of course, and benign tumors, are completely manageable.
Cancer is a group of diseases characterized by the autonomous and uncontrolled proliferation of malignant cells, with the ability to spread nearby and at a distance. Tumors are subject to the same rules of Natural Selection as any other living being. Cancer is subject to the evolutionary processes discovered by Darwin, realized through Natural Selection.
They start with non-lethal genetic and epigenetic changes in a single somatic cell of the organism, accompanied by the disruption of balances in proliferation, differentiation, and cell death, the formation of clones and subclones of tumor cells with genetic and epigenetic, consequently phenotypic changes among them, which is responsible for the heterogeneity within a cancer and among cancers of the same type. Genetic and phenotypic intratumoral heterogeneity, the variable pressure over time and space of the microenvironment, serves as a basis for the action of Darwinian Natural Selection, where cells that better adapt to the existing microenvironment in terms of securing food resources, reproductive ability, space occupation, and resistance to treatment, will be positively selected, thus favored, as a result, they will populate the tumor.
It is clear that cancer represents a mixture of cellular populations (clones and subclones) genetically and phenotypically different, competing for food resources and space, responsible for the progression of the disease and resistance to treatment. So cancer is not a single disease, it is not a homogenous mass like a benign tumor. Every cancer, due to intratumoral genetic and phenotypic heterogeneity, should not be treated as a single disease, but as a large number of diseases (as many as the number of clones and subclones within the same tumor). All this complexity can be explained with the classic principles of Natural Evolution.
Antitumor treatment is an artificial selective pressure on the dominant clone, opening space and food resources for less proliferative, yet more aggressive and treatment-resistant clones and subclones. Continuous genetic mutations (genetic instability) responsible for intratumoral heterogeneity represent the greatest obstacle to winning the battle against malignant metastatic tumor. Metastatic cancer remains the real challenge in tumor treatment.
Natural Evolution is the only developmental force of Life, one of the most powerful developmental forces on our Planet, Natural Selection is the "fairest judge" that exists on Earth. Darwin was the genius who managed, just through macroscopic observations (with the naked eye) and intuition, to present in 1859 one of the most brilliant ideas that human mind can produce: evolution of living beings, through Natural Selection.
The Natural Selection that Darwin discovered, unconsciously, automatically, blindly, essentially a non-random process, has "nothing in mind". It is systematic, always in action against every living being with the aim of developing the species to achieve the best possible fit to the constantly changing existing environment over space and time, practically achieving perfection that for the current time and conditions is the best possible, but it is endless. The goal is to increase survival chances for each individual of every species/cellular line, aiming also at achieving the possibility for reproduction.
Achieving reproduction is the only goal to ensure the transmission of the genome, thus ensuring the existence of the respective species/cellular line, as long as no living being is immortal.
The tumor is a disease only of multicellular organisms. It is a pathological cellular line for the “host” organism, originating from a single cell of this organism, its beginning and development are governed by the rules of Natural Evolution/Natural Selection, as for all other living beings. For normal cells, Natural Evolution aims at development, evaluated by us as positive; for pathological cells for humans (and for animals, birds, plants we care for), Natural Evolution also aims at their development, translated into; aggressiveness to capture as much space and food material as possible and resistance to treatment, that ensure survival and reproductive possibilities for the pathological cellular line itself, thus exceeding its genome.
But since these are done at the expense of normal cells and the very “host” (parasitic disease), thus harming human health (and that of animals, birds, plants we care for), we evaluate them negatively. Like every living being, malignant cells are in their “right” to survive (resistance, aggressiveness), reproduce (the main task is only the genetic contribution for the cellular line), to occupy spaces, only they do this at the expense of normal cells (from which they also originate) and the organism itself, but they do not “understand” that the death of the “host” organism is also their death.
Darwin did not have today's possibilities, but by studying cancer, you can imagine how Natural Evolution and Natural Selection begin and are realized much faster than in Nature. Scientists, doctors, mathematicians, geneticists, physicists had a ready theory, they have science, technique, but only 40 years ago (in 1976), Peter Nowell, proposed the clonal evolution of cancer and the application of evolutionary models to understand tumor growth, increase in aggressiveness, failure from treatment, that occurs during the natural history of malignant tumor.
A decade later, Nowell reflects that; “tumors arise from a mutated cell and biological and clinical progression is the result of additional genetic alterations (genetic instability), epigenetic consequently phenotypic, resulting in the formation of more aggressive subpopulations compared to the original malignant clone. Modern techniques of molecular, genetic studies, especially NGS (Next Generation Sequencing) have validated this theory.
The goal of treating any disease, including cancer, is its cure. It is not always achieved, especially for metastatic cancer. Cure means the elimination of the last tumor cell (one is enough to develop and reappear the malignant tumor). But to date, no one has been able to see how a normal cell transforms into a tumor cell in a multicellular organism and cannot evaluate the development of the tumor, without reaching at least 1,000,000 malignant cells (NGS with sensitivity 10-6) and for this reason, no one to date can evaluate how many tumor cells have remained below this number after treatment.
So no one can determine if the last malignant cell has been eliminated. And as long as you do not do this, you cannot tell a patient that his cure has been achieved and if the last tumor cell is not eliminated, any treatment regardless of its name, is considered palliative (alleviating a problem without dealing with the underlying cause).
If we could verify that the last malignant cell was eliminated, it is about the real cure of cancer. And if we had this result, there would be no need for further consolidative, maintenance treatments and monitoring of the patient. Only time will show if the real cure of cancer has been achieved (there will be no relapse of the disease).
The goal of antitumor treatment is to achieve Conventional Complete Remission (< 1 billion malignant cells), so the patient has no clinic, laboratory, radiological changes and the maximum so far Complete Molecular Remission (qPCR, NGS negative; < than 1 million malignant cells, probably also zero). If the latter is achieved, it is certain that the number of malignant cells is less than 1 million, it could be even zero (cure). As long as we cannot verify how many malignant cells have remained, consolidative, maintenance treatments, monitoring of the disease continue (especially in the first years after achieving this result). As long as we cannot verify, only maintaining this result for at least 10 years, with the Best Possible Quality of Life is considered “Operational Cure” = “Functional Cure, Minimal Residual Disease negative with NGS, but not necessarily zero malignant cells”.
Only time will verify the “Real Cure” (Eradication Cure, zero malignant cells). Cases where maintenance treatment is stopped and relapse does not occur (reappearance of the disease at any level of it), maybe (probably) are cases of “Real Cure” or where the minimum of remaining malignant cells manages to be kept under control by the Immune System of the “host”.
In the inability of these results, achieving Longevity and Quality of Life identical to that of people without the same disease of the same age, may be considered “cure”. In the treatment of metastatic malignant diseases, if real cure is not achieved (it cannot yet be determined), at least long-term disease control is aimed for (evidenced by stable responses to treatment), thus ensuring longevity and quality of life comparable to that of people without this disease, of the same age.
In the end, cured or not from a disease, death is inevitable, so the cure from any benign or malignant disease is relative.
Comparison of Intratumoral Heterogeneity, in different malignant tumors.
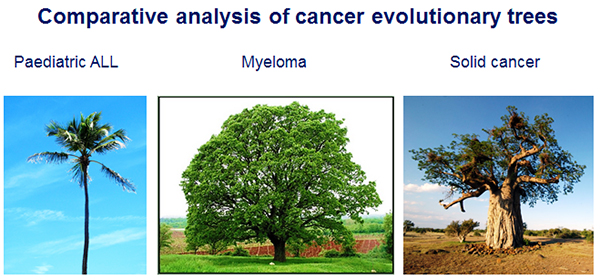
This figure presented by Prof. Gareth Morgan at the EMMA (European Multiple Myeloma Academy) meeting in 2012, was my first encounter with the fact that: “malignant tumors are subject to the same rules of Natural Selection as any other living being”.
Gareth Morgan, M.D. FRCP, FRCPath, Ph.D, Professor of Medicine, is the Director of the Myeloma Institute at UAMS. The UAMS (University of Arkansas for Medical Science) Myeloma Institute, under the leadership of Dr. Gareth Morgan, is the most comprehensive center in the world for research and clinical care related to multiple myeloma and related diseases.
Hello. I am 26 years old. Today marks 36 weeks and 3 days of pregnancy. For the past 2 months, I have been taking 1 tablet of iron a day and 1 Ferrodep capsule. Yesterday, I got my blood test results: WBC=9.64, RBC=3.8, HBG=11.6, HCT=35%, MCV=92, MCH=30.50, MCHC=33.10, PLT=199, LYM%=3.54%, MONO%=6.16, EO%=0.64%, BASO%=0.68%, Neut%=89%, LYM=0.34, MONO=0.59, EO=0.06, BASO=0.07, Neut=8.58, RDW-CV=14.40%, RDV-SD=39 fl, PDW=17, MPV=12.20, P-LCR=24%. Ferritin 14.34. My blood group is A+. Two months ago, my ferritin was 4.02 and hemoglobin was 10.3. I am continuing treatment but am concerned about the LYM which has significantly dropped in value (it was 16.26 two months ago, while at the beginning of the pregnancy it was within the normal range) and Neut% has slightly increased above the normal since the last time. What does this indicate? I am worried because yesterday I also had an ECG and it showed I have mild arrhythmia (I wore a Holter monitor and had about 4000 arrhythmias in 24 hours); the cardiologist told me that after giving birth, I will be followed up for 3 months and will be given medication. I have always been very active, working, going to the gym 5 times a week and during pregnancy I haven't had any issues with vomiting or difficulty breathing (except for the last 2 weeks where I have felt heavy and had some chest tightness) only anemia was a problem until now. Does the blood test indicate anything related to the heart?
Sent by Ina, më 22 April 2020 në 05:18
Hello Ina, you are currently considered to have an iron deficiency (ferritin < 20 ng/ml). The preparations you are taking will not correct the ferritin level. Use Ironorm 3 x 1 capsule/day, for at least 1.5 months, including after childbirth. Then repeat the ferritin test. The minimum normal value is 20 ng/ml and the optimal value is around 60 ng/ml
Replay from Dr. Shk. Sotiraq Lako, më 22 April 2020 në 10:08
Hello. I am 26 years old. Today I am 36 weeks and 3 days pregnant. For 2 months, I have been taking 1 tablet of tot'hema per day and 1 capsule of ferrodep. Yesterday I got my lab results: WBC=9.64, RBC=3.8, HBG=11.6, HCT=35%, MCV=92, MCH=30.50, MCHC=33.10, PLT= 199, LYM%=3.54%, MONO%=6.16, EO%= 0.64%, BASO%= 0.68%, Neut%= 89%, lym= 0.34, MONO=0.59, EO= 0.06, BASO= 0.07, Neut=8.58, RDW-CV= 14.40%, RDV-SD= 39 fl, PDW= 17, MPV= 12.20, P-LCR= 24%. Ferritin 14.34. I am blood group A+. Two months ago, my ferritin was 4.02 and hemoglobin was 10.3. Currently, I am continuing the treatment, but I am concerned about the lym which has dropped significantly in value (two months ago it was 16.26, while at the beginning of the pregnancy it was within the normal range) and neut% has slightly increased above the norm since the last time. What does this indicate? I am worried because yesterday I also did an EKG and it showed mild arrhythmia (I wore a Holter monitor and had about 4000 arrhythmias in 24 hours). The cardiologist told me that after giving birth, he would follow up with me for 3 months and prescribe medication. I have always been very active, working, going to the gym 5 times a week, and during the pregnancy, I haven't had any issues with vomiting or shortness of breath (except for the last 2 weeks when I felt heavy and had some chest tightness); only anemia was the problem until now. Does the blood test indicate anything about the heart?
Sent by Ina, më 22 April 2020 në 05:21
Hello Ina, you are currently considered to have an iron deficiency (ferritin < 20 ng/ml). The preparations you are taking will not correct the ferritin levels. Use Ironorm 3 x 1 capsule/day, for at least 1.5 months, including after childbirth. Then, recheck the ferritin levels. The normal minimum value is 20 ng/ml and the optimal value is about 60 ng/ml
Replay from Dr. Shk. Sotiraq Lako, më 22 April 2020 në 10:08
Hello Ina, you are currently considered to have an iron deficiency (ferritinemia < 20 ng/ml). The preparations you are taking will not correct the ferritinemia. Use Ironorm 3 x 1 capsule/day, for at least 1.5 months, including after childbirth. Then, repeat the ferritinemia test. The normal minimum value is 20 ng/ml and the optimal value is about 60 ng/ml
Replay from Dr. Shk. Sotiraq Lako, më 22 April 2020 në 10:08