Ear Diseases (Part Two)
Acute Mastoiditis

The most common complication of middle ear infections is mastoiditis, which means an extension of the infection from the middle ear cavity towards the pneumatic system of the temporal bone. In contrast to the development of the infection in the middle ear that concentrates on the mucosa, in the mastoid, we have bone dissolution.
Clinical Signs. Mastoiditis appears during the healing period of acute otitis and begins with an increase in temperature and worsening of the general condition, leukocytosis, and a significant increase in erythrocyte sedimentation rate.
Locally, we have a strong recurrence of pain in the ear synchronized with the pulse and radiating towards the mastoid and the occipital bone. Recurrence of odorless purulent discharges from the ear in larger amounts as well as hearing loss.
Pathogenesis.
- Acute middle ear otitis accompanied by mastoiditis generally reabsorbs without complications.
- The development of complications depends on the anatomical connections between the respiratory system and the tympanic cavity because a narrow passage between the antrum and the mastoid cells indicates poor aeration from the Eustachian tube.
- The virulence and resistance of the organism.
- The local resistance of the mucosa.
- The patient's overall immune situation.
- The patient's overall health condition.
Diagnosis.
- Purulent discharge from the ear.
- Strong pain when pressing the mastoid with a finger.
- Retroauricular edema accompanied by forward displacement of the earlobe.
Treatment. Inflammation that goes beyond the mucosa and is accompanied by bone tissue dissolution requires surgical intervention.
Indications for Mastoidectomy.
- In case of signs of intracranial complications.
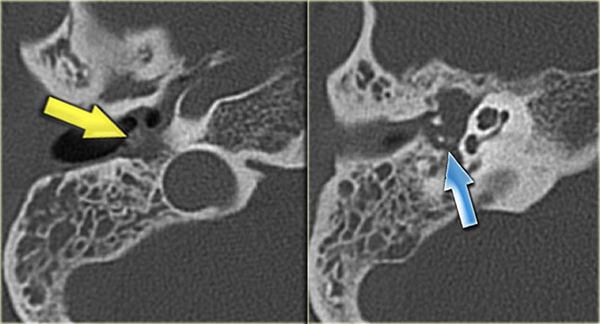
- Dissolution of the septa of mastoid cells and accumulation of pus in the space created, confirmed by CT.
- Appearance of facial paralysis.
The prognosis is good when the treatment is correct.
Chronic Middle Ear Otitis
Chronic middle ear otitis is divided into two types: Chronic mucosal inflammation and Chronic bone inflammation.
Chronic mucosal inflammation or mesotympanitis.

Clinical Presentation. We deal with chronic mucoid or purulent odorless discharge from the ear followed by intervals of calm but interrupted by acute re-infection episodes. The discharges are thick and purulent in the first phase and become mucoid and viscous as the infection begins to be absorbed. The patient complains about conductive or transmissive hearing loss, does not complain of pain, and is in good health condition.
Pathogenesis. The disease is not the result of a single cause but is the outcome of several different primary disease processes related to the middle ear. The inflammation remains confined to the mucosa.
Pathogenetic factors.
- Constitutional decrease in the self-healing ability of the mucosa.
- The type, pathogenicity, virulence, bacterial resistance.
- Anatomical situation in the middle ear cavity, such as pneumatization and the connections between the attic with the antrum, the middle ear cavity, and the Eustachian tube.
- Disorders of the Eustachian tube.
- General diseases such as allergies, immunological deficits, diabetes, etc.
Diagnosis. The anamnesis indicates a chronic discharge that repeats from time to time from the ear and is accompanied by hearing loss. In otoscopy, a central perforation of the tympanic membrane is observed, rarely we see a polyp as a result of mucosal hypertrophy from acute reinfections. CT shows a decrease in pneumatization and an increase in the opacity of the mastoid as a sign of chronic mastoiditis. The audiogram shows conductive hearing loss.
Treatment. When there is discharge, cleaning of the external ear canal is performed from time to time. Ear irrigation with body temperature physiological solution can be done. In the first phase, material is taken from the ear for antibiograms. Antiseptic solutions or those containing antibiotics but with no ototoxic effects are used for short periods.
In the dry phase of the disease, keeping the ear from water intrusion is advised as well as the immediate treatment of rhinopharyngitis. Surgical treatment includes mastoidectomy in cases when we want to eliminate the focus from the mastoid or tympanic cavity while tympanoplasty is performed with the aim of isolating the tympanic cavity and reconstructing the bone chain to prevent reinfections and improve hearing.
Chronic Bone Inflammation (Epitympanitis)
It is the result of a marginal defect of the tympanic membrane in the posterior-superior quadrant in the pars tensa or pars flaccida region. The infection spreads to the lateral part of the bone wall of the epitympanum. Granulations are common and are a consequence of bone osteitis.

Acquired cholesteatoma of the middle ear. Cholesteatoma involves the intrusion of the epidermis that covers the outside of the tympanic membrane through the perforation into the tympanic cavity, mainly in the attic. The creation of cholesteatoma is stimulated by reinfections of the tympanic cavity. The lateral perforation as a result of repeated infection causes osteitis of the lateral wall of the epitympanum in this place a pocket is created that accumulates epidermis which, growing, penetrates into the tympanic cavity.