Ear diseases (Part four)
Sigmoid sinus thrombosis originating from middle ear infections.
Clinical signs. An abscess of the perisinusal space, periphlebitis, and the beginning of sinus thrombosis closely resemble the epidural abscess. The detachment of infected thrombi creates the possibility of septicemias that include.

- Temperature with chills several episodes within the day.
- Tachycardia
- Headache
- Vomiting
- Drowsiness
- Neck stiffness
- Dyspnea in relation to metastatic pulmonary infections.
- Formation of metastatic hepatic abscesses.
Pathogenesis. The cholesteatomatous inflammatory process continues to destroy the surrounding bone walls and in some cases reaches the perisinusal space, causing the perisinusal abscess that leads to periphlebitis of the sigmoid sinus followed by sinus phlebitis. The thrombus initially forms on the sinus walls but gradually occludes its entire lumen and extends superiorly towards the sagittal sinus and below towards the internal jugular vein. The thrombus undergoes thrombolysis due to bacterial infiltration and creates the possibility of spreading small masses of the thrombus towards organs, creating the possibility of metastatic sepsis.
Diagnosis. Clinical signs in the setting of acute otitis or media with cholesteatoma that suggest sinus thrombosis.
- High temperature above 40 degrees C accompanied by chills throughout the day and not affected by antipyretics.
- Edema of the mastoid and strong pain on pressure at the level of its posterior border.
- Induration and tension of the jugular vein along the anterior border of the sternocleidomastoid muscle.
- In the septic form, petechiae are observed on the skin indicating blood clotting disorders.
- Splenomegaly
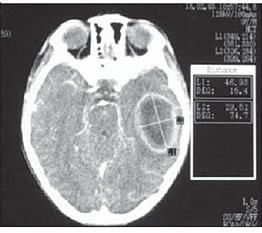
Radiological examinations. CT shows bone destruction in the sinus area. Angiography shows narrowing or occlusion of the sigmoid sinus in the venous phase of carotid angiography.
Differential diagnosis. This includes miliary tuberculosis, typhus, malaria, brucellosis, viral pneumonia, cystopyelonephritis.
Treatment. Immediate radical mastoidectomy revealing the sigmoid sinus to its healthy boundaries. The sinus is incised and cleaned from thrombi while the internal jugular vein is ligated and cut where there are no inflammatory phenomena. Antibiotic therapy with high doses and for a long period accompanied by anticoagulants.
Prognosis. The patient should be followed through repeated CTs to see changes in the surrounding tissues. The disease is fatal if not treated correctly or if the underlying cause and complications are not diagnosed in time. When treatment is started early, 80% of patients recover.
Otogenic cerebral abscesses.
It is one of the most serious complications that develop secretly in the terrain of a chronic cholesteatomatous inflammatory process of the middle ear.
Clinical presentation.
Initial phase. Meningism, nausea, headache, psychological changes, temperature.
Latent phase. Epileptiform attacks, neurological symptoms.
Clinical phase. Vomiting accompanied by bradycardia, behavioral disorders, aphasia, alexia, agraphia, hemiplegia, epileptic attacks, ataxia in cases of cerebellar abscess, cranial nerve paralysis, visual field disorders, oculomotor system and positioning disorders.
Terminal phase. Stupor, coma, eye deviation towards the lesion, bradycardia, and Cheyne-Stokes respiration.
Pathogenesis. The disease can spread through direct pathways.
- Through the tympanic tegmentum causing a temporal lobe abscess.
- Through the sigmoid sinus into the posterior cranial fossa causing a cerebellar abscess.
- Through the labyrinth into the endolymphatic sac forming a cerebellar abscess.
Another pathway is through the blood vessels (veins) or through the internal acoustic porus in cases of labyrinthitis.
Differential diagnosis. Should be made with tumors.
Treatment. The primary focus is removed through mastoidectomy and drainage of the abscess can be done at this moment, secondary removal can be done through craniotomy by a neurosurgeon. Radical elimination of the primary focus following the infection path is very important. High-dose antibiotics.
Prognosis. Even for cases that have received intensive surgical treatment, the mortality rate in developed countries remains at 5-8%.
Non-inflammatory diseases of the inner ear.
Otosclerosis.
Otosclerosis is a disease localized in the bony capsule of the labyrinth whose cause is still not discovered. The base of the stapes hardens as a result of being surrounded by spongy bone, this condition causes fixation of the stapes in relation to the inner ear so that the stapes can no longer vibrate normally.
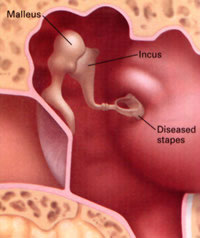
Otosclerosis can affect the stapes, malleus, and the bone surrounding the inner ear, resulting in the interruption of sound transmission to the inner ear. Untreated otosclerosis ends in complete deafness usually in both ears. The exact diagnosis is established by biopsy but only 10% of patients with histological changes present symptoms for otosclerosis.